COVID-19
On 11th March 2020 the World Health Organization declared the international spread of COVID-19 to represent a global pandemic. The unprecedented impact on the NHS and wider UK society led to the vast majority of clinical research being paused whilst all efforts and attentions were redirected to dealing with the pandemic. Recruitment to ROSSINI 2 at all sites was centrally paused on Friday 20th March 2020.
There will be long-reaching or even permanent changes to the NHS structures for delivering both patient care and clinical research as a result of COVID-19. As a result of these, we have slightly amended some trial processes and pathways in ROSSINI 2 to ensure safe and practicable reopening whilst protecting the scientific and methodological integrity of the trial.
These changes have been necessary in the following aspects of the trial: 1) secondary objectives; 2) trial entry criteria; 3) patient follow-up pathways. More detail on these can be found in the ROSSINI 2 Protocol V2.0
OBJECTIVE
To determine whether specific in-theatre interventions, alone or in combination, result in decreased rates of surgical site infection (SSI) up to 30 days post operation in adult patients undergoing abdominal surgery.
TRIAL DESIGN
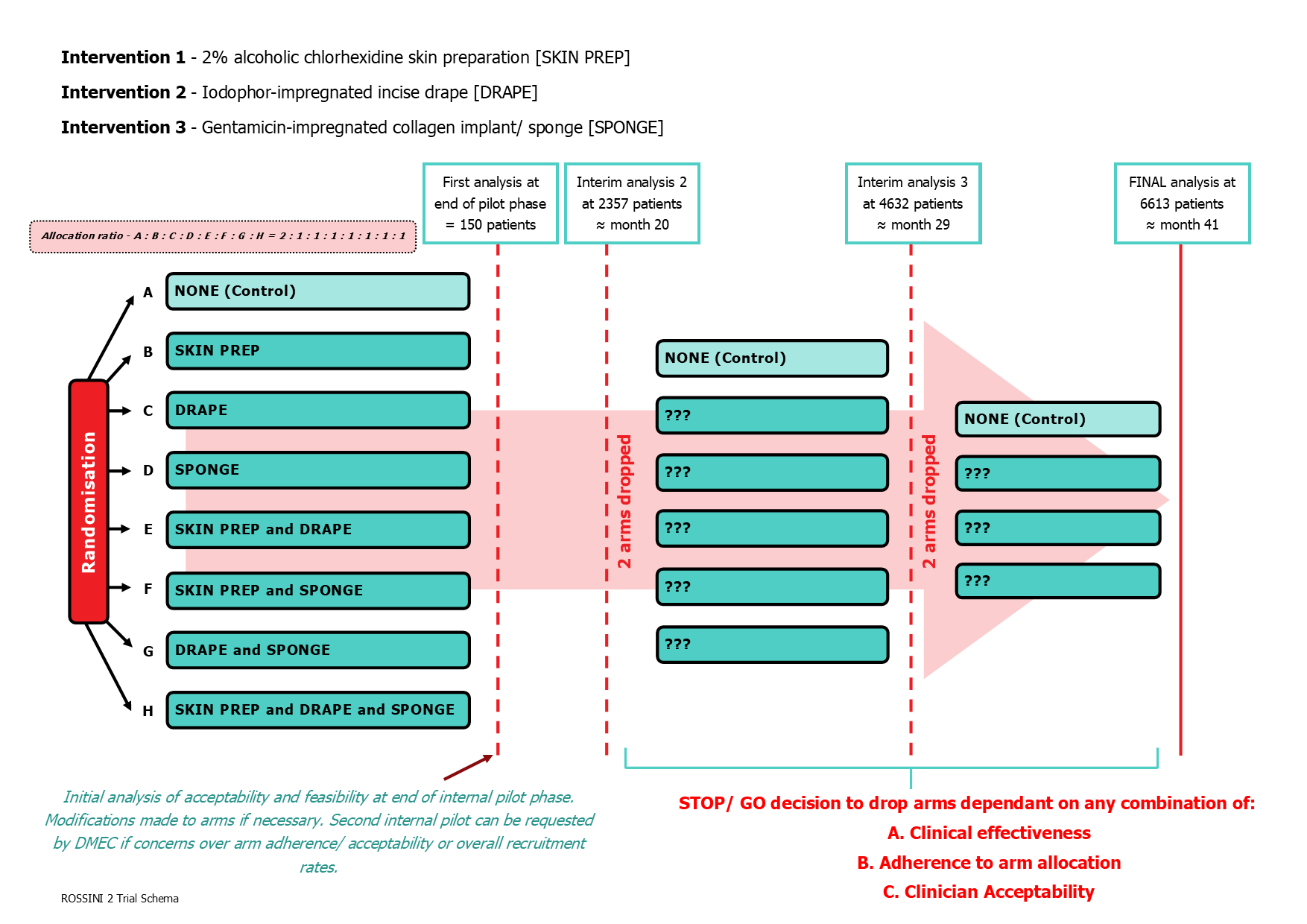
Multi-arm, multi-stage (MAMS) pragmatic, multicentre, randomised controlled trial, with an internal pilot, exploring the use of three separate in-theatre interventions to reduce SSI. A non-factorial design with allocation of various combinations of the three interventions to be used during the same operation, via either possible arms initially including a control arm.
PARTICIPANT POPULATION AND SAMPLE SIZE
6610 patients will be required to detect a 5% absolute risk reduction in the intervention arm(s) (15% to 10%) with 85% power.
ELIGIBILITY CRITERIA
Inclusion Criteria
- Patients undergoing an abdominal operation, these include colorectal, hepatobiliary, upper GI, urological, vascular, or gynaecological operations.
- Patients undergoing an abdominal operation (open or laparoscopic extraction site) with a planned incision of at least 5cm.
- Patients aged 16 years or older.
- Patients able and willing to undergo wound assessment (in person or remotely via telemedicine) at day 30-37 after surgery.
- Patients able and willing to give written informed consent.
- All contamination strata, including clean, clean-contaminated, contaminated or dirty surgery.
- Patients undergoing planned (elective or expedited) or unplanned (emergency) surgery.
Exclusion Criteria
- Previous laparotomy within 3 months prior to randomisation.
- Known to be pregnant or currently breast feeding.
- Operations where the wound is not anticipated to be closed primarily.
Notes on Eligibility Criteria
- SARS-COV-2 virus status and antibody status on day of surgery – all patients are eligible to enter the trial regardless of positivity, negativity or not tested status; this information is collected to allow us to control against these factors in the analyses.
- Patients with a new or documented allergy/ intolerance to any of the study interventions (chlorhexidine, iodine, collagen or gentamicin) will not be randomised to an arm containing this intervention, but will still be eligible for recruitment to other arms of the study.
- Patients with end-stage renal failure where gentamicin administration would otherwise be contra-indicated (according to local policy) will not be randomised to arms containing the gentamicin-impregnated sponge.
- Purely groin incisions such as inguinal hernia repair or vascular access of the femoral vessels do not count as abdominal surgery and are not eligible to enter the trial.
INTERVENTIONS
Three health technologies will be assessed versus their control arms (standard care):
- 2% alcoholic chlorhexidine skin preparation, versus any other standard skin preparation.
- Iodophor-impregnated incise drape, versus no drape.
- Gentamicin-impregnated implants/ sponge at closure, versus no implant/ sponge
OUTCOME MEASURES
Primary: Surgical site infection(s) up to 30 days post operation will be assessed by a trained blinded assessor, by patient’s self-report and defined according to the internationally accredited Centers for Disease Control and Prevention criteria (CDC).
Secondary:
- 30-day postoperative mortality rate (POMR).
- 30-day postoperative wound complication rate (Clavien-Dindo classification).
- Serious Adverse Events up to 30 days (wound or intervention-related only).
- Length of hospital stay after surgery as measured from the date of surgery to the date of discharge.
- Hospital re-admission for wound related complications within 30 days.
- Occurrence of unplanned wound reopening and/or re-operations within 30 days post-operation.
- Preference-based Quality of Life (QoL EQ-5D-5L) measured at Baseline, Day 7 (or discharge if sooner) and Day 30.
- Cost effectiveness (Resource Use Questionnaire (RUQ)).